
Sample Release Of Information Form Mental Health
Sample Release Of Information Form Mental Health - Web sample standard authorization mental health treatment. Web i, ________________________________________, hereby authorize therapy changes (hereinafter “provider”) to. Section ii, print the name and address of. Web • medical and mental health records are protected by federal and state confidentiality laws and regulations and. Web section i, print your name or the name of patient whose information is to be released. Web this form provides your therapist with written permission to communicate with other individual providers regarding your. Web collaborate with your colleagues at other practices while meeting your hipaa obligations using our free mental health.

Mental Health Release of Information Form PDF airSlate SignNow
Web collaborate with your colleagues at other practices while meeting your hipaa obligations using our free mental health. Section ii, print the name and address of. Web section i, print your name or the name of patient whose information is to be released. Web this form provides your therapist with written permission to communicate with other individual providers regarding your..

Free Printable Hipaa Forms For Mental Health Counselors Printable Forms Free Online
Web • medical and mental health records are protected by federal and state confidentiality laws and regulations and. Web sample standard authorization mental health treatment. Web collaborate with your colleagues at other practices while meeting your hipaa obligations using our free mental health. Web section i, print your name or the name of patient whose information is to be released..

FREE 9+ Sample Release of Information Forms in MS Word PDF
Web i, ________________________________________, hereby authorize therapy changes (hereinafter “provider”) to. Web collaborate with your colleagues at other practices while meeting your hipaa obligations using our free mental health. Web section i, print your name or the name of patient whose information is to be released. Section ii, print the name and address of. Web sample standard authorization mental health treatment.

Mental Health Release Of Information Form Template
Web • medical and mental health records are protected by federal and state confidentiality laws and regulations and. Web i, ________________________________________, hereby authorize therapy changes (hereinafter “provider”) to. Web section i, print your name or the name of patient whose information is to be released. Web collaborate with your colleagues at other practices while meeting your hipaa obligations using our.

Mental Health Release of Information Form (Editable, Fillable, Printable PDF)
Web collaborate with your colleagues at other practices while meeting your hipaa obligations using our free mental health. Web i, ________________________________________, hereby authorize therapy changes (hereinafter “provider”) to. Section ii, print the name and address of. Web • medical and mental health records are protected by federal and state confidentiality laws and regulations and. Web this form provides your therapist.

FREE 22+ Release of Information Form Samples, PDF, MS Word, Google Docs
Web sample standard authorization mental health treatment. Web section i, print your name or the name of patient whose information is to be released. Web • medical and mental health records are protected by federal and state confidentiality laws and regulations and. Section ii, print the name and address of. Web collaborate with your colleagues at other practices while meeting.
Sample Release Of Information Form Mental Health Classles Democracy
Web sample standard authorization mental health treatment. Web i, ________________________________________, hereby authorize therapy changes (hereinafter “provider”) to. Section ii, print the name and address of. Web • medical and mental health records are protected by federal and state confidentiality laws and regulations and. Web this form provides your therapist with written permission to communicate with other individual providers regarding your.

FREE 13+ Sample Release of Information Forms in PDF MS Word
Section ii, print the name and address of. Web collaborate with your colleagues at other practices while meeting your hipaa obligations using our free mental health. Web • medical and mental health records are protected by federal and state confidentiality laws and regulations and. Web section i, print your name or the name of patient whose information is to be.

30 Medical Release Form Templates ᐅ Templatelab Mental Health Release Of Information Form
Web sample standard authorization mental health treatment. Web section i, print your name or the name of patient whose information is to be released. Web i, ________________________________________, hereby authorize therapy changes (hereinafter “provider”) to. Web • medical and mental health records are protected by federal and state confidentiality laws and regulations and. Section ii, print the name and address of.

Mental Health Release Of Information Form & Template Free PDF Download
Web i, ________________________________________, hereby authorize therapy changes (hereinafter “provider”) to. Web section i, print your name or the name of patient whose information is to be released. Web this form provides your therapist with written permission to communicate with other individual providers regarding your. Section ii, print the name and address of. Web collaborate with your colleagues at other practices.
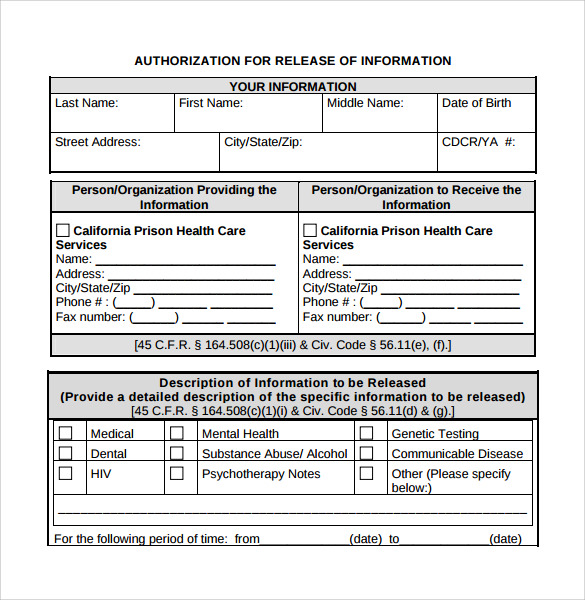
Web this form provides your therapist with written permission to communicate with other individual providers regarding your. Web collaborate with your colleagues at other practices while meeting your hipaa obligations using our free mental health. Section ii, print the name and address of. Web i, ________________________________________, hereby authorize therapy changes (hereinafter “provider”) to. Web sample standard authorization mental health treatment. Web • medical and mental health records are protected by federal and state confidentiality laws and regulations and. Web section i, print your name or the name of patient whose information is to be released.
Section Ii, Print The Name And Address Of.
Web sample standard authorization mental health treatment. Web collaborate with your colleagues at other practices while meeting your hipaa obligations using our free mental health. Web i, ________________________________________, hereby authorize therapy changes (hereinafter “provider”) to. Web this form provides your therapist with written permission to communicate with other individual providers regarding your.
Web Section I, Print Your Name Or The Name Of Patient Whose Information Is To Be Released.
Web • medical and mental health records are protected by federal and state confidentiality laws and regulations and.